Mechanical ventilator manual link designed: https://drive.google.com/file/d/1uRV9ktVYHOwRvqs9B8ZddRuZ2AVFL2I7/view?usp=sharing
Mechanical Ventilator
BackGrounds
A ventilator is a machine designed to mechanically move air in and out of the lungs to intermittently or continuously assist or control pulmonary ventilation, This device is primarily used in intensive therapy to help improve the patients breathing by regulating the flow of gas in the lungs.
Objectives of the design of a Mechanical Ventilator
- Supply control of ventilation.
- Enable the exchange of gases.
- Reduce respiratory work.
- Facilitate muscle recovery (weaning).
- Allow sedation, anesthesia
Basic Concepts
 |
| Figure 1: general scheme of operation of a uci ventilator |
 |
| Figure 2: Patient Breathing Circuit
In an intensive care ventilator (ICU) we use oxygen and high pressure air. Once filtered, the pressure of each gas is reduced and stabilized to an optimum value, and then each one is dosed separately by means of proportional valves, in order to obtain the gas mixture in the amount and proportion necessary to ventilate to the patient. This is achieved by insufflating said gas during the inspiratory phase.
|
Mechanical Ventilation Modes
Conventional Ventilatory Modalities:
- Assist-Control Ventilation (ACV) : Total assisted-controlled mechanical ventilatory support is the most basic form of MV, it is used in those patients who present a considerable increase in ventilatory demands and who therefore need total replacement of ventilation. The assisted-controlled modality allows the patient to initiate the cycling of the ventilator starting from a preset value of respiratory frequency (f) that ensures, in the event that this one does not make inspiratory efforts, the ventilation of the patient.
- Synchronized Intermittent-Mandatory Ventilation (SIMV): The synchronized intermittent mandatory ventilation allows the patient to perform spontaneous breaths interspersed between the mandatory cycles of the ventilator, the word synchronized refers to the waiting period that the ventilator has before a mandatory cycle to synchronize the inspiratory effort of the patient with the insufflation of the ventilator. When used with high f covers the patient's ventilatory demands, being comparable to conventional assisted-controlled ventilation. Used with low frequencies, the SIMV allows the progressive disconnection of the Mechanical Ventilation (VM).
- Pressure-Controlled Ventilation (PCV) - Pressure Support Ventilation (PSV): It is an assisted modality, limited to pressure and cycled by flow, which modifies the spontaneous ventilatory pattern, that is, it decreases the respiratory rate and increases the circulating volume. The ventilator provides a ventilation aid, programmed from the support pressure level. The pressure remains constant throughout the inspiration, and in parallel the flow decreases progressively until reaching the level that allows the start of expiration. This partial support modality is widely used, since it allows to synchronize the respiratory activity of the patient with the ventilator when responding to changes in the patient's ventilatory demand. In addition, it preserves respiratory work and reduces the need for sedation and healing, thus facilitating the disconnection of the VM.
- Peep: Positive end-expiratory pressure (PEEP) is a mechanical technique that is often used when ventilating an unconscious patient. This technique includes the addition of a quantity of pressure in the lungs at the end of each breath. The patient's ventilation process causes a degree of desufflation in the lungs; between breaths, the lungs contain less air than usual. By adding positive pressure at that time, we try to reinfuse the respiratory tract.
- Continuous Positive Airway Pressure (CPAP): It is a spontaneous breathing modality with PEEP, in which a supraatmospheric pressure is maintained throughout the ventilatory cycle. The flow must be high to guarantee a high gas supply, higher than the requirements of the patient and small pressure oscillations (<5 cm H2O) so as not to cause excessive respiratory work.
- Airway Pressure Release Ventilation (APRV): It combines the positive effects of continuous positive airway pressure (CPAP) with the increase in alveolar ventilation obtained by the transient decrease in airway pressure from the level of CPAP to a lower level. Ventilation with pressure release provides long periods of insufflation, interspersed with brief periods of pulmonary deflation. It is a mode of partial ventilatory support cycled by the ventilator or by the patient and in which during the period of insufflation the patient can breathe spontaneously. Its main advantage lies in the fact that the pressure in the airway can be set at a modest level, and furthermore as the pressure is maintained during a longer period of the respiratory cycle an alveolar recruitment occurs. In theory, short periods of deflation do not allow alveolar collapse, but it is sufficient for the exchange of gases not to be affected by the CO2 clearance.
Respiratory Curves: in the different ventilation modes mentioned above, flow, pressure and volume curves are used in time to have a detailed analysis of the operation of the mechanical ventilator.
 |
| Figure 3: Respiratory Curves (flow,pressure and volume) |
According to figure 3:
Flow Curve: Starts according to the flow pattern selected at the beginning of inspiration. In assisted or pressure-controlled respirations, the flow is slowed and in volume-oriented modalities, quadratic flow is generally used. At the end of the inspiration, the flow becomes 0, and is inscribed below the X axis, which represents the expiration that constitutes the most important portion of the curve, it must be linear starting from the maximum expiratory flow to the baseline, before of the next breath (expiratory pause time). In the different ventilation modes mentioned above, flow, pressure and volume curves are used in time to have a detailed analysis of the operation of the ventilator.
Volume Curve:Should be correlated with the previous ones, indicates some of the problems already mentioned in the previous curves.
Pressure Curve:This should ascend smoothly. In ventilations controlled by the ventilator, the pressure curve starts from the final expiratory pressure and in those triggered by the patient, an initial negative inscription indicates the inspiratory effort. In the pressure curve the autopeep is not observed because it is disguised, it must be suspected when the inspirations begin very early on the expirations (high respiratory frequency) or the patient has conditions having autopeep (bronchial asthma, COPD, small caliber tube).
Design
Interface Desing

 |
| Figure 4: Design Control panel |
The design of the mechanical ventilator for adults was developed through the implementation of an interface called the control panel, where the ventilatory control modes are selected, parameters are entered and the respiratory curves are observed. everything named above is implemented in the LabView programming software.
Electric Diagram
 |
| Figure 5: Electric Diagram Mechanical Ventilator |
 |
| Figure 6: Mechanical Ventilator Electric Block Diagram
the mechanical ventilator consists of two control modes that are pressure and volume, in the pressure mode, the inspiratory time value is entered, which is an important consideration to take into account when ventilatory support is started, giving the relation between the duration of inspiration and expiration. dynamic parameters are established as the maximum and minimum pressure known as PEEP, the range of pressure was established between 40-100 mmHgO, which in the theory corresponds to 5-30 cmH2O, the results to be obtained will be the pressure and volume curves, where the volume is a function of the pressure.
For the volume control, parameters such as maximum volume and minimum volume are established, the volume control carries an inspiration-expiration relationship through the control or implementation of flow. At the beginning of the mechanical ventilation, a flow must be established that ensures an inspiratory time of around 1 second (0.8-1.2 s), which is equivalent to programming a peak or maximum flow of about 60 l / min (40-80 l / min), but in the design made the system flow is constant In this case the volume control is determined taking into account pressure parameters, the volume range was established between 50 and 600 ml.
The ventilatory system has a self-test as verification test of ventilator operation, in which auditory alarm operation, patient detection, patient breathing system in operation is reviewed. On the other hand, it has two auditory and visual alarm systems. The visuals are observed as LEDs on the control panel, the alarm systems are due to high pressure and valve obstruction.
Programmed Design  
The programming in LabView consists basically of three buttons that are the selection to the self-test, control pressure and volume control, which is then directed to a cycle while doing three processes, insufflation, time of inspiration, expiracion and inspiration, annexed to this is find the programming of the alarms with conditionals.
Mathematical Desing
Pressure

Figure 6: Linearization Pressure

Figure 7: Linear Regression Pressure
Volume

Figure 6: Linearization Volume

Figure 9: Linear Regression Volume
The previous linearizations observed in Figure 8 and 9, are made to implement the equation of the line obtained in the programming within each of the cycles.
The pressure linearization was obtained by measuring the voltage at different pressure values, which was indicated by the manometer. for the volume as it was reacted as a function of pressure, the maximum voltage was taken at a maximum pressure and the minimum voltage at a minimum pressure and each one at a volume value.
Results
Control Pressure
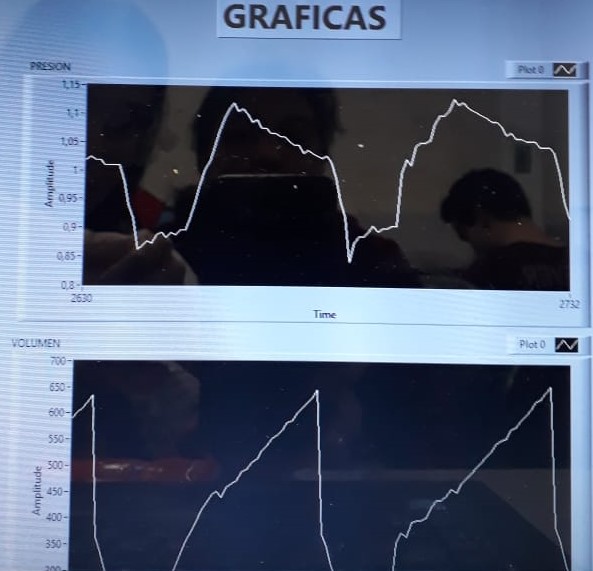
Figure 10: Curves Control Pressure
Pressure wave: It is written starting from zero or the value of the PEEP as an upward wave during inspiration until reaching the maximum pressure. An inspiratory pause can be seen if programmed, then falls during expiration to the level of the final expiratory pressure. The respiratory effort is inscribed as a negative deflection before the wave described.
Volume wave: In it, leakages or leaks are observed well, when the expiratory wave does not reach the baseline.
Control Volume

Figure 11: Curves Control Volume
The pressure limit of each cycle increases or decreases depending on the circulating volume of the previous cycle. A certain VT and the advantages of the pressure controlled are ensured, since they limit the pressure in the adjusted value. Figure 11 shows the inspiration and expiration without inspiratory pause in the volume graph.
Conclusions
Bibliography
MacIntyre, NR., et al. Mechanical Ventilation, 2nd ed.
2009.
Marco Ranieri, Rocco Giuliani, Tommaso Fiore, Michele Dambrosio, Joseph Milic-Emili. Volume-Pressure Curve of Respiratory Sistem Predicts Effects of PEEP in ARSD: Occlusion versus Contant Flow Technique. Am J Respir Crit Care Med.; Vol 149. pp 19-27, 1994.
Benito S.: Sustitución total de la ventilación. En: Net A, Benito S, eds. Ventilación mecánica. 3ª ed. Barcelona: Springer-Verlag Ibérica; 1998.
|
T
No hay comentarios.:
Publicar un comentario